[ Home Page ] [ Site Map ]
Hodgkin's Lymphoma
Classification
Clinical Features
Laboratory Diagnosis
Cytogenetics
Molecular Genetics
Transformation and Progression
Treatment and Prognosis
- Classical Hodgkin's Lymphoma
- Nodular sclerosis (grades I & II)
- Mixed cellularity
- Lymphocyte-rich
- Lymphocyte depletion
- Nodular Lymphocyte Predominant Hodgkin's Lymphoma
The distinction between Hodgkin's Lymphoma (HL) and other types of lymphoma has its origin over a century ago long before there was any concept of the cellular basis of the disease. Until recently it was not clear how HL was related to other types of haematological malignancy. It is now recognised that both main subtypes of Hodgkin's lymphoma are types of B-cell lymphoma. The relationship with other types of B-cell lymphoma is further illustrated by the occurrence of composite lymphomas where the tumour has characteristics of Hodgkin's lymphoma and Diffuse Large B-cell Lymphoma, B-CLL or Follicle Centre Lymphoma.

Classical Hodgkin's Lymphoma
- majority of cases present with lymphadenopathy which has a contiguous pattern
- stage distribution at presentation approximately equally distributed between localised (stages I & II) and advanced (stages III & IV) disease
- mediastinal disease in approximately 50% of cases, associated with nodular sclerosing histology
- systemic B-symptoms and abnormalities of haematological parameters (anaemia, lymphocytopenia, raised ESR) in up to 30% of cases is associated with aggressive histological subtypes
- peak age incidence in 3rd decade
- sex ratio (M:F) approximately 1.3:1
- alcohol intolerance in about 2% of cases.
Nodular Lymphocyte Predominant Hodgkin's Lymphoma
- localised disease in >80% at presentation (usually involving single node)
- systemic symptoms rare (about 5%)
- male predominance (M:F 4:1)
- peak age incidence 4th decade
- common sites of disease include suprahyoid neck and inguinal lymph nodes.
Morphology
Classical Hodgkin's Lymphoma
I) Nodular sclerosis:
- characterised by nodular growth pattern and birefrigent collagen band formation. Capsular fibrosis frequently seen.
- a cytological spectrum of diseases ranging from an abundance of lymphocytes with scanty Hodgkin's Reed-Sternberg (H-RS) cells to a lymphocyte-depleted appearance with abundant tumour cells.
- predominant morphology of the H-RS cells is the lacunar cell, characterised by lobulated nucleus, prominent eosinophillic nucleolus and abundant clear cytoplasm.
- grading system divised by British National Lymphoma Investigation recognised 2 grades: an
aggressive subtype (Grade II) characterised by 25% or more of cellular nodules showing lymphocyte depleted or pleomorphic cytological features. All other cases including borderline cases categorised as grade I (low grade).
II) Mixed cellularity:
- classical Hodgkin's Lymphoma lacking histological features which would otherwise permit classification as a specific subtype.
III) Lymphocyte-rich classical Hodgkin's Lymphoma:
- lymphocyte-rich cellular background containing typical H-RS cells, maybe nodular or diffuse.
- when nodular, it is characterised by expanded mantle zone regions colonised by H-RS cells. There is a relative paucity of H-RS cells, histiocytes, plasma cells and eosinophils.
IV) Lymphocyte depletion:
- includes diffuse fibrosis and reticular Hodgkin's disease from the Lukes and Butler classification.
- now very rarely diagnosed, and it is recognised that many cases previously diagnosed as HD (lymphocyte-depletion) are in fact examples of non-Hodgkin's lymphoma, commonly of anaplastic large cell type Anaplastic Large Cell Lymphoma.
- the majority of cases of show morphological features of diffuse fibrosis characterised by a hypocellular background containing bizarre H-RS cells and associated with non-collagenous fibrosis.
Nodular Lymphocyte Predominant Hodgkin's Lymphoma
- may show partial or total nodal effacement by a nodular, or nodular and diffuse proliferation of small lymphoid cells.
- a characteristic H-RS cell variant is present termed the L&H (or 'popcorn') cell characterised by a lobulated and twisted nucleus, and a nucleolus which is typically smaller than that seen in H-RS cells of Classical HL.
- the number of popcorn cells is variable and may comprise up to 10% of the cellular population within the nodules. Collagenous fibrosis is uncommon.
- classical H-RS cells are extremely rare and are not required for the diagnosis.
Immunophenotype
Classical Hodgkin's Lymphoma
- H-RS cells frequently express CD30 and CD15 (80% of cases)
- expression of CD20 on a minor sub-population of H-RS cells in up to 2/3 of cases
- vast majority of cases show expression of a 55kD actin-bundling protein termed FASCIN in the H-RS cells.
- evidence of Epstein-Barr virus either by LMP1 immunohistochemistry or by EBER in situ hybridisation in up to 30% of cases in UK
- lymphoid population shows a predominance of CD4+ peripheral T-cells adjacent to the H-RS cells, around which they may form rosettes.
Nodular Lymphocyte Predominant Hodgkin's Lymphoma
- nodules are composed of mantle zone B-cells expressing IgM and IgD, with admixed follicular dendritic cells
- L&H cells have a B-cell phenotype expressing CD20 and CD79a, and show evidence of immunoglobulin-synthetic capacity with expression of cytoplasmic J-chain
- epithelial membrane antigen is frequently expressed by the L&H cells
- numerous T-cells are also present with a CD4 predominance, some co-expressing the germinal centre-associated T-cell marker CD57. T-cells form rosettes around the L&H cells.
 |
 |
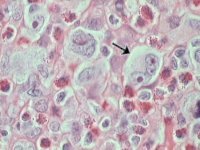
Nodular sclerosing HL: H&E stained lymph node section showing Lacunar cell morphology (arrowed). |
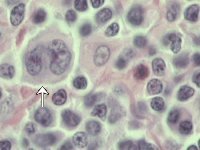
Mixed cellularity HL: H&E stained lymph node showing Reed-Sternberg cell morphology (arrowed). |
 |
 |
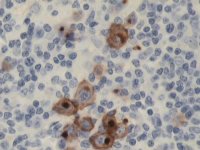
Mixed cellularity HL: Reed-Sternberg cells stained by CD15 immunoperoxidase. |
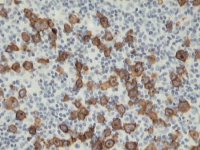
Mixed cellularity HL: CD30 immunoperoxidase stain. |
The cytogenetics of both Classical HL and the rare cases of Nodular Lymphocyte Predominant HL which have been karyotyped show complex numerical and structural abnormalities affecting all chromosomes, with as yet no identifiable non-random cytogenetic abnormality.
- molecular genetic analysis of micro-dissected single H-RS cells from cases of classical HL demonstrate clonal hypermutated immunoglobulin heavy chain genes with 'crippling' mutations.
- similar analysis of L&H cells from cases of Nodular Lymphocyte Predominant HL show somatically hypermutated immunoglobulin heavy chain genes without crippling mutations and ongoing antigen-driven hypermutation in an identical fashion to the Follicle Centre Lymphomas.
Classical HL
- relapsing cases have a tendency to increase the numbers of H-RS cells present which maybe associated with depletion of lymphoid cells
- the development of secondary NHL occurs in about 0.8% of cases at 25yrs.
Nodular Lymphocyte Predominant HL
- relatively high frequency of developing secondary NHL (3.8% at 25yrs), most of which are diffuse large B-cell lymphoma, but rare cases of peripheral T-cell lymphoma have been described.
- the development of secondary non-Hodgkin's lymphoma is usually associated with multiple relapses.
The prognosis of HL has improved dramatically over the last 30 years. Treatment is dependant on the stage at presentation and the presence of systemic symptoms. The majority of patients in current studies in the UK receive combination chemotherapy. Patients with localised (stages I & II) asymptomatic disease may be treated with radiotherapy alone.
[inline image: survival curve]
Current therapies for HL may be associated with a variety of long-term side effects which include sterility, secondary leukaemias and epithelial malignancies.
[ Home Page ] [ Site Map ]
Copyright © HMDS 1999-2005
Document last updated:
Tuesday, 18 November 2003
Comments & feedback to:
[email protected]
[URL: www.hmds.org.uk/hl.html]